
Part 21 of 49 - Video Presentations of the "1st Conference on Integrating Early Detection of Heart and Lung Disease through Low-Dose CT": Day 1 Session 3: Reinventing Public Health in the Era of AI
- Jan 27, 2025
- 17 min read
Thursday, September 19, 2024 | New York Academy of Medicine (NYAM)
1216 5th Ave, New York, NY 10029
Dr. Cheryl Healton, DrPH, emphasizes the role of AI in public health, particularly in expanding lung screening and managing smoking-related illnesses. She discusses the rising global smoking rates, especially among women and adolescents, and warn of an impending surge in lung cancer and other diseases. Dr. Healton also draws attention to the complexity of changing health behaviors, and the potential of AI tools to improve health outcomes. Healton also highlights the importance of equitable AI applications and addressing socioeconomic barriers to ensure effective health interventions.
Watch Dr. Cheryl Healton's Presentation Below:

See Dr. Cheryl Healton's Slides Below:


































-
Transcript of Dr. Cheryl Healton's Presentation:
[Cheryl Healton] [0.56s] Good afternoon, everyone.
[Cheryl Healton] [1.84s] How are you?
[Cheryl Healton] [4.88s] We're gonna move to the big, big, big picture now for just a little while.
[Cheryl Healton] [9.04s] That's how my, my talk is focused, Reinventing Public Health in the Era of AI, harnessing information to expand lung screening and to save lives.
[Cheryl Healton] [17.52s] I think we have a formidable challenge before us.
[Cheryl Healton] [19.91s] I think any of you in the audience that were also in Madrid remember some of the discussion that we had there.
[Cheryl Healton] [25.84s] So this this map is a map of the world, and it gives you the percentage of people who are presently smoking as of 2021, who are aged 15 or higher.
[Cheryl Healton] [35.49s] And that little graph there goes from 0% to 37%.
[Cheryl Healton] [40.05s] If this were broken out between men and women, it is not.
[Cheryl Healton] [42.77s] That's a blend.
[Cheryl Healton] [43.95s] We'd have a higher, risk rate there.
[Cheryl Healton] [47.48s] So in other words, more men smoke than 37% in many places, sadly.
[Cheryl Healton] [52.59s] What does this mean?
[Cheryl Healton] [53.80s] It means if you remember the slide we saw earlier today about the tsunami, we have upcoming tsunami of lung cancer and of all of the other smoking related illnesses and, of course, of the other causes of lung cancer, which in some places are becoming more prominent because of the decline for those who are at the other end of the tsunami, like the United States, with respect to lung cancer.
[Cheryl Healton] [77.58s] But the tsunami is still waiting to come in some places based on them having reached their peak in smoking fairly recently, and it is still yet to come in countries whose actual tobacco baseline rate and their population rate are still stabilizing in that.
[Cheryl Healton] [95.83s] In some countries, population is declining, surprisingly so, and in others, it's rising at a lower rate than had previously been expected.
[Cheryl Healton] [103.98s] All of those dynamics will affect the size and the nature of the tobacco related illness tsunami.
[Cheryl Healton] [109.98s] The next slide, if I can Looks again and we we talked about this in Madrid.
[Cheryl Healton] [117.27s] We don't use the term developed countries, underdeveloped countries.
[Cheryl Healton] [120.31s] We use now low middle income countries and also the Human Development Index.
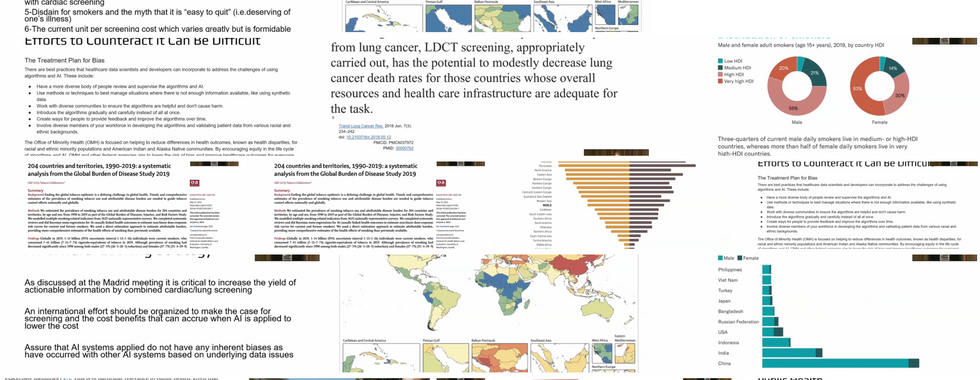
[Cheryl Healton] [125.19s] So these these circles are based on the Human Development Index.
[Cheryl Healton] [128.75s] They're male and female.
[Cheryl Healton] [130.50s] I have one main take home message from this.
[Cheryl Healton] [133.22s] If you look at the, percentage of the very high, human development index for how many smokers there are, you'll see for men, 20% 53%.
[Cheryl Healton] [149.65s] Distribution of smokers blah blah blah blah.
[Cheryl Healton] [151.97s] Okay.
[Cheryl Healton] [152.45s] I'm getting I'm confusing myself.
[Cheryl Healton] [154.37s] But, basically, the opportunity that is there for the tobacco industry is enormous with respect to women.
[Cheryl Healton] [161.38s] And so if we think that we've seen the peak in many countries, we have not because we have many countries in which very slow very low proportions of women smoke.
[Cheryl Healton] [170.34s] And the the numbers that are smoking are rising while they are falling among men and among other populations, including, countries where zoo we've gone from 0 adolescents to 1% adolescents to as much as 14 percent of adolescents in as little as 5 for 6 years.
[Cheryl Healton] [187.75s] So, again, the nature of the tsunami remains largely unpredictable due to a number of factors.
[Cheryl Healton] [194.94s] And one of those factors is the extent to which the tobacco industry will endeavor to get the market that they're not getting.
[Cheryl Healton] [203.80s] And an example is that I always like to give is a Philip Morris ad showing a beautiful African woman in African garb and across her neck in written in Swahili the following sentence.
[Cheryl Healton] [212.03s] Find your voice.
[Cheryl Healton] [214.22s] Following sentence, find your voice.
[Cheryl Healton] [217.92s] That was a shot heard around the world because, of course, smoking is one of the primary ways that women will lose their voice.
[Cheryl Healton] [224.38s] But in in Africa, some four countries have Swahili as their main language and other 14, speak it.
[Cheryl Healton] [230.77s] This was a very powerful ad from Philip Morris moving through Africa to try to get a population whose smoking rates were exceptionally low.
[Cheryl Healton] [240.13s] Next.
[Cheryl Healton] [242.03s] By country, countries with the most smokers from the bottom up.
[Cheryl Healton] [245.95s] As you can see, this has been, a problem originally largely of high income countries, but it has moved into low and middle income countries substantially.
[Cheryl Healton] [257.24s] And, again, this is a building tsunami in countries where the access to care, is even is even lower and the ability to marshal screening resources probably also will remain lower.
[Cheryl Healton] [272.50s] So, in this particular overview, I just wanna bring home a few key points and that is globally in 2019, 1.4 1,000,000,000 individuals were current smokers.
[Cheryl Healton] [284.82s] It's a little bit higher than that right now.
[Cheryl Healton] [287.22s] It's 1 in 8, 1 1 in 8 world smoking, prevalence.
[Cheryl Healton] [294.66s] The that translates into tobacco accounting for 7,690,000 deaths and 200,000,000, disability life years per year.
[Cheryl Healton] [304.95s] It is the leading risk factor for death worldwide.
[Cheryl Healton] [309.03s] It has been the leading cause of death worldwide since I entered public health in about, let's see.
[Cheryl Healton] [315.20s] How back 1974, 75?
[Cheryl Healton] [319.20s] So that's many, many years ago, and it has not lost its place yet as the leading cause of of, tobacco related death.
[Cheryl Healton] [326.64s] It's distributed in various ways.
[Cheryl Healton] [328.64s] This is a distribution of smoking among males, and the color code is simply the dark red and the greens are the higher rates, and the yellow and the blues are the lower rates.
[Cheryl Healton] [340.88s] And as you can see, the epidemic is waning in certain parts of the world that used to have very high smoking rates and and building up in other parts of the world.
[Cheryl Healton] [352.14s] And the same is also true for women as well.
[Cheryl Healton] [355.83s] And this one shows the actual code, proportion of all cause deaths that are related to tobacco.
[Cheryl Healton] [361.75s] In the blue, it's under 5%, and in the red, of which there's very little on the female slide, but if we were to go back to the male, there's more red there.
[Cheryl Healton] [371.66s] In the red, you'll see that it is 30 to 35 percent of all deaths caused by tobacco, which kind of startles people, understandably.
[Cheryl Healton] [383.68s] And then by country, the incidence and the mortality.
[Cheryl Healton] [388.31s] I always in presenting this to a public health audience, I first let everyone know that in the last century, 100,000,000 people died of tobacco.
[Cheryl Healton] [396.82s] And then I say, how many people do you think are going to die in this century?
[Cheryl Healton] [400.10s] And I let everyone guess in the class, and never, not once yet, have I gotten the right answer.
[Cheryl Healton] [405.22s] In this audience, I know the right answer is here.
[Cheryl Healton] [407.46s] What's the right answer?
[Cheryl Healton] [408.66s] How pardon?
[Cheryl Healton] [411.44s] No.
[Cheryl Healton] [411.76s] How many how many people will die of tobacco related causes in this century versus the 100,000,000 that died in the last century?
[Cheryl Healton] [425.48s] Well, way more.
[Cheryl Healton] [427.00s] The question is how much more?
[Cheryl Healton] [430.92s] Okay.
[Cheryl Healton] [431.24s] I'm not hearing the answer, Earl.
[Cheryl Healton] [433.32s] Yes.
[Cheryl Healton] [433.72s] Exactly right.
[Cheryl Healton] [434.44s] Over a 1000000000.
[Cheryl Healton] [435.56s] Who who said over a 1000000000?
[Cheryl Healton] [437.28s] Take a bow because it's a it's it's an answer that very few people know.
[Cheryl Healton] [442.00s] I want you to state that right off the bat.
[Cheryl Healton] [444.56s] And it's also very helpful when you're explaining an epidemiologic problem to a school of public health class is to have them understand the correlation between incidence and mortality, not only how many people get a die of it, which is, of course, very high with lung cancer.
[Cheryl Healton] [458.50s] They're getting somewhat more optimistic, but also the framework within which that happens.
[Cheryl Healton] [463.06s] If it's Ebola, it's close to a 100% within a very short time frame.
[Cheryl Healton] [467.49s] If it's lung cancer, it's within a few years if you're stage 4 if you're not lucky enough to be getting the absolute highest quality of care.
[Cheryl Healton] [475.17s] So now here is currently a p AI currently being applied in public health.
[Cheryl Healton] [482.67s] Public health treats the population.
[Cheryl Healton] [485.15s] Those of you who are clinicians in this room, treat the individual.
[Cheryl Healton] [488.99s] Everything you do as clinicians affects population health and everything population health does in terms of its decision making, which would be something like how do the insurance companies cover screening or not and which groups do they cover.
[Cheryl Healton] [503.06s] That is, quote, the public health policy level.
[Cheryl Healton] [506.04s] AI is becoming a very important tool within public health, but there is considerable suspicion about it within public health because of the extent to which if they get it wrong, they get it wrong in a big way.
[Cheryl Healton] [518.28s] And so these are the these categories, those are the core categories of what the field of public health is responsible for in the United States of America, health promotion, health surveillance, health protection, population health assessment, disease and injury prevention, emergency prediction preparedness and response.
[Cheryl Healton] [538.12s] I've left it out of this discussion, the last one, because I don't think it's terribly relevant to what we're talking about today, but health promotion, policies and services to maximize cessation with AI tools.
[Cheryl Healton] [548.36s] We just heard a little bit about that, and we also heard about it in relation to dietary modification.
[Cheryl Healton] [554.00s] The development of those tools will be extraordinarily important with respect to the work that you plan on doing with an integrated CT with respect to demonstrating the actual cost benefit or cost effectiveness and that, of of that integrated strategy.
[Cheryl Healton] [570.68s] Because if you have the integrated strategy and, yes, you do a surgical intervention on lung cancer one time because someone's stage whatever, and that person goes right back out and continues to smoke and stops bothering to screen, you have a whole other, cost benefit than if you are actually able to integrate that person into a system that will stay with them for as long as it takes for them to quit.
[Cheryl Healton] [594.35s] I will make one point here right now because I've heard the term lifestyle factors and behavioral factors multiple times since I came here.
[Cheryl Healton] [601.51s] You rarely hear those words within a school of public health.
[Cheryl Healton] [605.51s] And the reason you don't is that the theoretical underpinnings of public health have evolved to think in terms of the social determinants of health, and the data have suggested that these simple lifestyle changes, even the concept of simple lifestyle changes, in reality, it is not simple.
[Cheryl Healton] [623.70s] It does not happen easily.
[Cheryl Healton] [625.94s] And just even in my period as leading a foundation dedicated to reducing smoking in America, the fact that I kept driving home that nicotine was addictive and that indeed is considered the most addictive substance known to humankind, reframed the way people felt about their own, addiction to nicotine and to various tobacco products, and it also reframed the way their family thought about them.
[Cheryl Healton] [650.44s] So the one thing that I would say is as you take on this big challenge of doing the screening that integrates multiple illnesses and then you say, okay.
[Cheryl Healton] [659.27s] Now we know you're at risk for this, you're at risk for that, you're at risk for that.
[Cheryl Healton] [662.88s] Here's how you want we want you to change.
[Cheryl Healton] [665.36s] You cannot manage that on your own.
[Cheryl Healton] [666.96s] And I've heard some people say you can't because of time and reimbursement.
[Cheryl Healton] [670.17s] Fine.
[Cheryl Healton] [670.65s] But even if you had all the time and reimbursement in the world, it would not be something that you would want to manage because it is not an easy task.
[Cheryl Healton] [679.61s] Changing people's weight in fact, you probably all know the literature short of the new miracle drugs that we we see now, making that change extremely difficult.
[Cheryl Healton] [688.41s] The metabolism recalibrates and at a at a much lower caloric level still continues to keep its weight.
[Cheryl Healton] [695.38s] It creates a new homeostasis, and it adopts that homeostasis and moves forward.
[Cheryl Healton] [700.01s] So all of these things are extremely complicated.
[Cheryl Healton] [702.27s] And then I'll add one more that as I was putting it together, I thought it's really important to make this point.
[Cheryl Healton] [708.91s] The people who still smoke in the world, particularly in the high income countries, That behavior is highly correlated with poor diet, substance use, and independent of the substance use, the excessive alcohol use.
[Cheryl Healton] [724.10s] And so you are going to find, when you start doing your studies, very high between all of these problems.
[Cheryl Healton] [730.42s] So it's not just that there's a behavioral target that needs to be addressed.
[Cheryl Healton] [734.18s] There could be multiple simultaneous behavioral targets to address.
[Cheryl Healton] [737.94s] And I don't need to tell you.
[Cheryl Healton] [739.30s] I'm sure you can imagine on your own how complex that is.
[Cheryl Healton] [742.97s] I raise that because I think the AI tools are extraordinary additions to our ability to be able to manage that, manage it in a cost effective way, manage it in a fairly relentless way, study the impact of being relentless because at some point someone shuts you down and says, I don't want your messages anymore.
[Cheryl Healton] [762.33s] I don't want your calls.
[Cheryl Healton] [763.45s] I don't want your advice.
[Cheryl Healton] [764.97s] But we have seen great effect with these tools.
[Cheryl Healton] [767.13s] I'll give you one example developed by our own group at Legacy and then also at NYU is taking someone who quit smoking and giving them a tool where they can never walk by a store that's selling cigarettes, which previously and in most states still are plastered with advertisements for various brands on the front of the store.
[Cheryl Healton] [787.29s] In some jurisdictions, that's not permitted, but in many parts of the country, the south in particular is still very common.
[Cheryl Healton] [792.89s] So that was a great advantage for people who are trying to quit smoking to not have to walk by where they could buy cigarettes 15 times a day in any given day.
[Cheryl Healton] [801.44s] Health surveillance, integrated databases to assess patterns and prevalence of smoking.
[Cheryl Healton] [806.88s] So we not we not only need to know who is smoking, we need to know where they're smoking, how much they're smoking, why they're smoking, and then we have a whole new pattern emerging in terms of the pattern of the disease pattern associated with smoking because people are doing a mix of different products.
[Cheryl Healton] [823.17s] Health protect protection, assessing policies that work through AI tools.
[Cheryl Healton] [827.33s] I'll give you a great example.
[Cheryl Healton] [828.38s] I work for the White House Office of Drug Control Policy.
[Cheryl Healton] [831.17s] Yesterday, it was announced there was a near 11% 1 year decline in opioid related deaths.
[Cheryl Healton] [837.98s] Yes.
[Cheryl Healton] [838.38s] Don't clap too soon because it was there are there are some reasons why it may be correct.
[Cheryl Healton] [843.22s] There are some reasons why it may be higher than it is.
[Cheryl Healton] [847.06s] However, in the period in which that happened as a result of of efforts undertaken by the Biden administration, multiple policy changes happened all at once.
[Cheryl Healton] [857.59s] That's an AI problem of considerable import.
[Cheryl Healton] [861.59s] So you have 50 states, 50 different opioid epidemic trajectories, 50 different rates of decline or increase that occurred during that 12 months.
[Cheryl Healton] [870.44s] And nothing would be more wonderful than to be able to say of those 10 initiatives that happened all over the country and were implemented at various levels in in different places, which one or ones and what combination are really driving this decline?
[Cheryl Healton] [886.88s] There are anecdotal explanations about what's driving it.
[Cheryl Healton] [890.08s] Naloxone becoming, OTC being one of them.
[Cheryl Healton] [893.37s] That's lovely.
[Cheryl Healton] [894.16s] But very large swath of swaths of pharmacies will not stock it because they don't want those people entering their pharmacy.
[Cheryl Healton] [902.03s] I would mandate that every pharmacy has to stock it.
[Cheryl Healton] [904.43s] I wouldn't let them be able to opt out of a life saving drug, but that's in fact what's happening.
[Cheryl Healton] [909.07s] So AI can be extraordinarily powerful at the policy and health surveillance level and the health protection level.
[Cheryl Healton] [916.50s] And then population health assessment, detect the prevalence, at the population level and the affinity to the standard of care.
[Cheryl Healton] [923.97s] Here's a very important issue.
[Cheryl Healton] [926.77s] I mean, if all of you are doing this kind of screening, what assurance, short of you being involved in a tight study where you must have the insurance assurance to produce the data, in the general practice of your screening, how many of you really know what happened with regard to the risk factor that you're tracking, if you are tracking it, of the patient you advised to do x with their weight, y with their smoking, z with their drinking.
[Cheryl Healton] [954.32s] And the answer is probably the answer is probably very few of you know what happened with those things.
[Cheryl Healton] [962.48s] And if you do know, you may be, because this is the norm, report relying on self report.
[Cheryl Healton] [968.83s] I won't say it's notoriously, unreliable, but it is definitely somewhat unreliable.
[Cheryl Healton] [974.36s] So in a in a in a sense, it's wonderful to identify the problem, but on the other side of that, you want to understand the solution.
[Cheryl Healton] [983.40s] Okay.
[Cheryl Healton] [984.28s] AI.
[Cheryl Healton] [985.56s] This is a picture of, from California.
[Cheryl Healton] [988.60s] They're not protesting against AI.
[Cheryl Healton] [990.44s] They're protesting against the death of George Floyd, but the article covered the relationship between discrimination and AI.
[Cheryl Healton] [1001.74s] And I probably am not telling any of you something you don't know, but it is extremely important for us to track how AI algorithms are put together and what inherent problems they may have that can lead to systematic biases associated with them.
[Cheryl Healton] [1019.87s] And the office of minority health at the national level in in HHS has had a group that summarized what they viewed as some of the key things that need to occur.
[Cheryl Healton] [1031.65s] If you read up on AI, and I'm no AI expert as I as I told David when he asked me to do this talk, you you hear about the, quote, black box, which is the data in, the advice or the conclusions about what should happen out, and how frequently the people involved in implementing the advice on the out outer end of that black box cannot explain the logic model of how that truism occurred.
[Cheryl Healton] [1061.96s] Okay?
[Cheryl Healton] [1062.61s] So these are these are the recommendations to at least begin to take great care in how you approach the application of AI, particularly by creating a system that is systematically biased against women, systematically biased against one minority group or another, systematically, biased against an ethnic group that has a different pattern of disease.
[Cheryl Healton] [1089.38s] And it it it explains how to do it.
[Cheryl Healton] [1091.14s] I won't read them all, but I will say that I think they're critically important to consider.
[Cheryl Healton] [1096.92s] And this example, here, I will simply just read from the most important section.
[Cheryl Healton] [1102.76s] For example and many of you probably saw this paper.
[Cheryl Healton] [1105.64s] It got many headlines that led to the Commonwealth Fund making a major contribution to watching for this problem.
[Cheryl Healton] [1112.23s] For example, an algorithm used in hospitals to allocate health care services to patients in the United States was found to be biased against black patients.
[Cheryl Healton] [1120.23s] Among black and white patients who were equally sick, black patients were assigned lower risk scores and were therefore less likely to receive additional services.
[Cheryl Healton] [1128.48s] This bias arose because the algorithm was designed to protect health care costs rather than illness.
[Cheryl Healton] [1134.32s] As black patients tended to have poor access to care, they also tend to cost the health care system less, and their insurance tends to cover less.
[Cheryl Healton] [1142.26s] And so when you have systems that are seeking to advise on care based on insurability or you're using data based on the care pattern that was based on insurability, you can have some important systematic difficulties.
[Cheryl Healton] [1158.10s] Then a paper that was written in 2018, let's hope he's wrong for the coming decades, and I know we all know him Paul Pinsky.
[Cheryl Healton] [1166.14s] While tobacco control remains the most important tool in the long term to decrease morbidity and mortality from lung cancer, LDCT screening appropriately carried out has the potential to modestly decrease lung cancer death rates for those countries whose overall resources and health care infrastructure are adequate for the task.
[Cheryl Healton] [1185.18s] That was 2018.
[Cheryl Healton] [1187.18s] Our goal, I would assume, is not to settle for modest, but look on the horizon at 2018 as sensible, a modest reduction in wealthy countries.
[Cheryl Healton] [1197.56s] I would say we would love to see, you know, a modest to large reduction everywhere in the world, by the application of AI appropriately, with appropriate guardrails on the AI that it's legitimate and has no systematic biases built into it.
[Cheryl Healton] [1215.48s] Apply that on a on an international basis in a way that will save lives.
[Cheryl Healton] [1220.63s] What are what are the things that stand in the way of that?
[Cheryl Healton] [1223.67s] What are the challenges?
[Cheryl Healton] [1225.12s] Resources, resources, resources that came up over and over, especially in LAMCs where the priorities compete with so many other things, so many other basic things that are not happening.
[Cheryl Healton] [1235.35s] So you're saying, oh, do these special things for people who smoke too much, but, that may crowd out vaccines or other basic, care for basic services.
[Cheryl Healton] [1245.03s] So that creates a a catch 22 in attention.
[Cheryl Healton] [1248.83s] Demand.
[Cheryl Healton] [1249.47s] People do not know about the option, and health care providers are not offering the option even in wealthy countries.
[Cheryl Healton] [1255.31s] I know that because I know so many recent quitters for for whom no one ever mentioned screening to them.
[Cheryl Healton] [1261.16s] They're very shocked when I say you really should get a CT.
[Cheryl Healton] [1263.64s] Where is that?
[Cheryl Healton] [1264.36s] Why should I do that?
[Cheryl Healton] [1265.48s] They're not being told.
[Cheryl Healton] [1266.36s] Hence, the litigation and the class action suits that are starting around this.
[Cheryl Healton] [1269.80s] I think some of you may have seen the ads which are on constantly in Washington, DC.
[Cheryl Healton] [1274.91s] Fear, forever an issue.
[Cheryl Healton] [1276.28s] Fear and trust.
[Cheryl Healton] [1277.47s] Not trusting the system and not wanting to know.
[Cheryl Healton] [1280.36s] These are key issues that are well documented in the literature.
[Cheryl Healton] [1283.71s] Human resources, even in well off countries.
[Cheryl Healton] [1286.03s] The reason, the ability to to crank out without the use of a radiologist results for large numbers of scans that you're going to be excluding in this system.
[Cheryl Healton] [1295.36s] That's a great opportunity to be to conserve human resources and expand what can be done.
[Cheryl Healton] [1301.82s] Disdain for smokers and the myth that it's easy to quit, in essence, blaming them for not only their behavior, quote, behavior, but all future illnesses that may flow from it.
[Cheryl Healton] [1312.13s] The current, unit cost per screening, which varies greatly across the world, I certainly learned that in Madrid.
[Cheryl Healton] [1318.67s] That's a major obstacle.
[Cheryl Healton] [1320.11s] It's everything's relative.
[Cheryl Healton] [1321.23s] If it's $35 in Egypt, it's still a huge amount of money in Egypt, $35 compared to the 3 or $500 in this year.
[Cheryl Healton] [1328.43s] And the guideline itself, in my opinion, I think that opinion is shared, is too narrow.
[Cheryl Healton] [1333.23s] I'm talking about the federal guideline.
[Cheryl Healton] [1335.63s] A forward looking strategy, as we discussed at the Madrid meeting, it's critical to increase the yield of actionable information by combined cardiac, lung, and I guess now I'm going to say liver and everything else, osteoporosis screening.
[Cheryl Healton] [1348.52s] And international efforts should be organized to make the case for screening and the cost benefits that can accrue when AI is applied to produce this lower cost, including the lower cost of the behavioral interventions, which I think are truly key to demonstrate the efficacy of what you're doing.
[Cheryl Healton] [1365.49s] Assure that AI systems applied do not have any inherent biases that have occurred in other AI systems.
[Cheryl Healton] [1371.73s] And marketing, sort of a dirty word on some level, but I don't feel that way because the foundation I led unsold cigarettes to adolescents really quite thank you.
The presentations were hosted by I-ELCAP – The International Early Lung Cancer Action Program.



Comments