



Part 12 of 49 - Video Presentations of the "1st Conference on Integrating Early Detection of Heart and Lung Disease through Low-Dose CT": Day 1 Session 2: Emphysema and COPD
- Jan 10, 2025
- 7 min read
Updated: Jan 10, 2025
Thursday, September 19, 2024 | New York Academy of Medicine (NYAM)
1216 5th Ave, New York, NY 10029
Dr. Albert Rizzo, MD, Chief Medical Officer for the American Lung Association, emphasized the importance of early detection and consistent treatment for COPD and emphysema. He highlighted the need for clear definitions and guidelines, noting that many patients remain undiagnosed and untreated. In addition, he addresses the debate over the use of CT scans in COPD diagnosis and treatment, noting both their potential benefits and limitations. Dr. Rizzo also discussed the potential benefits of new drugs and the importance of involving pulmonologists in patient care to improve outcomes and reduce healthcare costs.
Watch Dr. Albert Rizzo's Presentation Below:

See Dr. Albert Rizzo's Slides Below:














-
Transcript of Dr. Albert Rizzo's Presentation:
[Albert Rizzo] [0.16s] Thank you for inviting me to be here.
[Albert Rizzo] [2.00s] I'm a pulmonologist and the chief medical officer for the American Lung Association.
[Albert Rizzo] [6.16s] And to my cardiology colleagues, congratulations on your 100th anniversary.
[Albert Rizzo] [10.32s] Lung Association's also having an anniversary this year of a 120 years.
[Albert Rizzo] [16.98s] 19 0 4 as the Society to Prevent Tuberculosis.
[Albert Rizzo] [19.79s] So that got changed later in the 19 forties when antibiotics or TB came about.
[Albert Rizzo] [24.90s] It's still a problem worldwide.
[Albert Rizzo] [26.27s] In this country, it's under better control.
[Albert Rizzo] [28.38s] But I I mentioned the years because public health agencies have to be in it for the long game.
[Albert Rizzo] [33.10s] Hopefully, tomorrow, you're gonna hear more about implementation, policy changes.
[Albert Rizzo] [37.02s] It's been 60 years since the surgeon general's report on tobacco and lung cancer and lung disease.
[Albert Rizzo] [42.55s] 60 years, and we still have majority of our states have very little in the way of tobacco control laws.
[Albert Rizzo] [48.40s] It's also been about, 54 years since the Clean Air Act went into play.
[Albert Rizzo] [53.57s] We still have the, tug of war between industry and public health regarding ozone and particle pollution.
[Albert Rizzo] [59.97s] So this is a long game for all us all of us.
[Albert Rizzo] [62.45s] We also know it takes a long game to get into practice.
[Albert Rizzo] [66.69s] Practice patterns change slowly.
[Albert Rizzo] [68.36s] Doctors don't like to change their habits.
[Albert Rizzo] [70.53s] Despite the fact that guidelines are made based on standards of care, they're not implemented the same everywhere.
[Albert Rizzo] [77.17s] Excuse me.
[Albert Rizzo] [78.05s] So tomorrow would be a lot that we can talk about as far as implementation and policy.
[Albert Rizzo] [83.54s] Emphysema and COPD.
[Albert Rizzo] [85.30s] The word emphysema is gonna mean a lot of different things to different people.
[Albert Rizzo] [88.50s] Pathologists see it differently.
[Albert Rizzo] [89.94s] Radiologists see it differently.
[Albert Rizzo] [91.62s] Physiologists have a different definition.
[Albert Rizzo] [93.94s] Primary care doctors, we have 5 of them.
[Albert Rizzo] [96.02s] You'll probably get variation in answers.
[Albert Rizzo] [99.22s] And I think a patient, when they see it in their patient portal, is gonna have a very different understanding of what the word emphysema means.
[Albert Rizzo] [105.53s] So we have to get on the same page about what do you do when a patient has, quote, emphysema on a report.
[Albert Rizzo] [111.65s] And emphysema does not equate to COPD.
[Albert Rizzo] [115.33s] Can I go to the next slide, please, or do I do that?
[Albert Rizzo] [118.45s] Top green.
[Albert Rizzo] [119.25s] Top green.
[Albert Rizzo] [119.89s] Okay.
[Albert Rizzo] [121.17s] Alright.
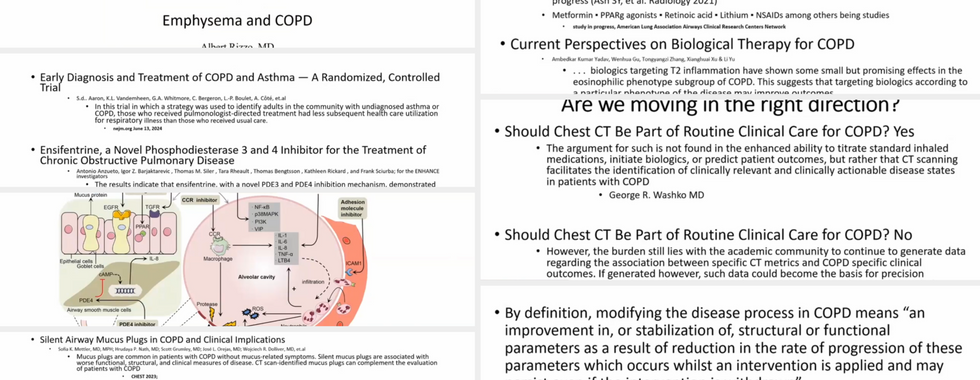
[Albert Rizzo] [121.81s] So the, the 2 paragraphs there, these are articles from CHEST back in 2018.
[Albert Rizzo] [129.49s] So 6 years ago, 2 well known pulmonary specialists, Meilan Hahn and George Washko, who've been doing a lot of work with COPD gene and spiromix, had this, point counterpoint discussion, should COPD have CT scans as part of routine care?
[Albert Rizzo] [144.97s] And I think if you look at them both, they would say the CT scans have utility in the treatment of patients with COPD, not necessarily at that time when they're talking about COPD helping to be diagnosed with CT scan.
[Albert Rizzo] [159.39s] But the bottom line was that, George felt that more information you had, the better.
[Albert Rizzo] [164.43s] You may find things that are not related to the suspected COPD in this patient, so the more information is good.
[Albert Rizzo] [170.99s] Meilhan took the approach that we don't have a whole lot of evidence that finding, things on a CT scan early in a patient with COPD or a patient already with diagnosed COPD, what can we do differently about it?
[Albert Rizzo] [182.81s] In other words, can we modify the disease?
[Albert Rizzo] [184.97s] And as she says, the academic community, and at this point hopefully the pharmaceutical industry, are moving to look at ways of modifying the disease, that we call COPD, which again is not the same thing as emphysema.
[Albert Rizzo] [199.05s] But why is it important to report emphysema and related findings?
[Albert Rizzo] [202.25s] So put a few articles here.
[Albert Rizzo] [203.93s] Some of them are very well known to you, some authored by David and and Claudia, but it's starting to tell us that if you see things on a CT scan that you weren't necessarily suspecting, there are gonna be some things to do about it.
[Albert Rizzo] [216.15s] It also tells you that these findings have an implication as to what the patient's outcome is gonna be.
[Albert Rizzo] [221.70s] Increased mortality from respiratory disease in undiagnosed, emphysema or COPD.
[Albert Rizzo] [228.10s] And if these scans can at least lead the primary care doctor to getting pulmonary function studies in patients, it may improve the fact that of the 12 to 15000000 patients with COPD in this country, there's another 12 to 15000000 who are not diagnosed with COPD, which means they're not getting the recommendations to be on, guideline directed therapy, They're not getting the smoking cessation effects that, they should be getting.
[Albert Rizzo] [253.25s] They're not doing the exercise they should be getting.
[Albert Rizzo] [255.41s] And I'm gonna mention an article later on where simple things such as identifying the COPD and acting early can make a difference in quality of life.
[Albert Rizzo] [265.00s] And modifying the disease, this is a definition from, I think, NIH in 2009, really just means slowing down the process.
[Albert Rizzo] [272.92s] It's nice if you could reverse it, but slowing it down, stabilizing it, and improving the functional status of the diseased patient.
[Albert Rizzo] [280.67s] And most of the drugs we have now over the last 40 years are symptom control inhalers.
[Albert Rizzo] [285.07s] Most of them help the patient get through the day.
[Albert Rizzo] [287.39s] They don't necessarily slow down the progress of the disease.
[Albert Rizzo] [291.63s] But I think we are moving to a point where we're starting to see some benefit in that regard.
[Albert Rizzo] [296.19s] Now the first article I have cited here is from a recent New England Journal, from a Canadian group where they did some case finding.
[Albert Rizzo] [304.55s] They looked at a population that had COPD with or without symptoms, and what they decided to do is let's find the patients who, were not being seen or diagnosed with COPD, diagnose them with pulmonary function, and then send half of them to a pulmonary specialist and the other half to primary care physician.
[Albert Rizzo] [324.03s] In this country, most of the patients with COPD are treated by primary care physicians.
[Albert Rizzo] [328.43s] But as was alluded to earlier today and we talked about tomorrow, they have a lot on their plate.
[Albert Rizzo] [332.81s] Primary care physicians have diabetes, cardiac disease, rheumatoid arthritis, osteoporosis, plus COPD on their plate.
[Albert Rizzo] [339.53s] Many physicians today still have some nihilism and stigma around COPD because of the smoking related aspect of it.
[Albert Rizzo] [346.25s] We all know that COPD is not just caused by smoking.
[Albert Rizzo] [349.66s] But what this study found was if they had a pulmonologist see the patient, put them on some guideline directed therapy, these patients had less exacerbations, better quality of life, and lower health care utilization over the course of the study, meaning less cost to society.
[Albert Rizzo] [364.41s] The second article on this page is a fairly new drug that was released by the, approved by the FDA, which is a PDE 3 and 4 inhibitor.
[Albert Rizzo] [373.53s] Now this goes to the point that c d o p d is an inflammatory disease.
[Albert Rizzo] [377.13s] Mentioned it earlier today in cardiology.
[Albert Rizzo] [378.96s] Almost everything on our body that's a disease has to do with in some way with inflammation, including cancer.
[Albert Rizzo] [384.56s] The tumor microbiome has a lot of immunology involved with it.
[Albert Rizzo] [388.49s] So this is a drug that is now slowing down the inflammation in these patients and improving the quality of life.
[Albert Rizzo] [394.15s] And I think we need to continue down this road of trying to improve the disease modifying process.
[Albert Rizzo] [400.31s] There's a study this top one is being conducted by the American Lung Association's ACRC or airways, airway centers for respiratory for control research control.
[Albert Rizzo] [411.59s] And, what they're doing is putting several different drugs through a study to see if they modify the disease process of emphysema.
[Albert Rizzo] [420.22s] The last article on this page is looking at all the biologic drugs that can be potentially, developed and have targets, and this is my last slide, which looks complicated, but what it's just trying to show you that the the milieu of cytokines, molecules, cells that are playing a role in COPD all could be potential targets to nip this in the bud.
[Albert Rizzo] [440.64s] So if we find a patient that has emphysema reported on the CT scan, they can at least be told the essential h that was mentioned earlier today, get off their cigarettes, stay healthy.
[Albert Rizzo] [450.76s] They should at least get pulmonary functions done if they haven't had them done.
[Albert Rizzo] [454.04s] If they're diagnosed with COPD, they go down the road of getting standard, guideline therapy directed preferably by a pulmonologist if the PCP doesn't have the time to do it.
[Albert Rizzo] [463.67s] And with that, I will stop.
[Albert Rizzo] [465.43s] Thank you.
The presentations were hosted by I-ELCAP – The International Early Lung Cancer Action Program.



Comments