
Video Presentations of the "1st Conference on Integrating Early Detection of Heart and Lung Disease through Low-Dose CT": Day 1 - Welcome and Introduction by Dr. David Yankelevitz
- Dec 27, 2024
- 24 min read
Thursday, September 19, 2024 | New York Academy of Medicine (NYAM)
1216 5th Ave, New York, NY 10029
Dr. David Yankelevitz emphasized the significance of integrating lung cancer screening with cardiology, marking a new era in preventive health. He highlighted the importance of reporting all clinically relevant findings from CT scans, a practice that has evolved significantly with AI. The conference aims to foster collaboration between cardiology and lung health experts, optimize screening protocols, and address ethical considerations. Dr. Yankelevitz also acknowledged the contributions of various organizations and the recent recognition of Dr. Claudia Henschke's work in early detection.
Watch Dr. David Yankelevitz's Presentation Below:

See Dr. David Yankelevitz's Opening Slides Below:




















-
Expand to Read the Text Transcript
Transcript of Dr. Claudia Henschke's Introduction and Presentation:
Jump to Dr. Morteza Naghavi's Presentation
Jump to Dr. David Yankelevitz's Presentation
[Dr. Claudia Henschke] [0.80s] Welcome to the, 1st conference on integrating early detection of heart and lung diseases and the 46th international conference on screening for lung cancer.
[Dr. Claudia Henschke] [12.88s] We've been doing this for a long time and the 14th conference on the initiative on for early lung cancer research on treatment.
[Dr. Claudia Henschke] [20.89s] So as I said, we started in 1992, to talk about screening.
[Dr. Claudia Henschke] [26.41s] It took us until 1998 to really recruit a 1,000 people, which we did, and and that resulted in The Lancet publication in 1999.
[Dr. Claudia Henschke] [37.29s] And then all people were starting, were were becoming interested.
[Dr. Claudia Henschke] [43.74s] I wanna remind you that it all started at Weill Cornell with Dean Gatto at the head.
[Dr. Claudia Henschke] [48.95s] And the senior, you know, when I initially tried to get through the IRB, never went through the IRB, but Jim Smith, the senior pulmonologist, went with me to the IRB, and we got it through in 10 minutes after after that.
[Dr. Claudia Henschke] [62.68s] Mark Basementier was a senior oncologist and doctor Alturkey.
[Dr. Claudia Henschke] [66.19s] Nasser Alturkey was a thoracic surgeon, and David Skinner was the president.
[Dr. Claudia Henschke] [70.92s] And it took that was the initial team.
[Dr. Claudia Henschke] [73.80s] It took all of that team to make it work.
[Dr. Claudia Henschke] [78.97s] So we then expanded to the International ILCAP, and I'm proud to say we've now screened a 102,000 participants in ILCAP in more than 80 institutions around the world, and we're still growing.
[Dr. Claudia Henschke] [97.37s] So thank everybody for all of that.
[Dr. Claudia Henschke] [101.61s] It's throughout the world, and we're expanding into new continents of Africa and, South America, which I'll talk about at the other talks.
[Dr. Claudia Henschke] [113.97s] So we were finally through that collaboration, we were able to give the 20 year lung cancer specific survival, which was really very terrific.
[Dr. Claudia Henschke] [123.83s] It was a 80% for all comers whether diagnosed through the screening or inter in between screening rounds, baseline or annual.
[Dr. Claudia Henschke] [133.13s] And if you found it in the earliest, stage, pathologic stage, the survival was 95%.
[Dr. Claudia Henschke] [140.65s] So, really, that's outstanding.
[Dr. Claudia Henschke] [142.09s] So we can really cure lung cancer if we keep working towards that and finding it earlier and earlier.
[Dr. Claudia Henschke] [148.01s] And that's one of the purposes of this meeting.
[Dr. Claudia Henschke] [151.06s] We wanna thank, Louis doctor Luis Sejo from the Universidad de Navara.
[Dr. Claudia Henschke] [157.38s] They were one of our first institutions that joined us, and he hosted the our last conference in Madrid.
[Dr. Claudia Henschke] [165.21s] And we thank Mateus Utkirk for, suggesting the agile collaboration and the agile planning team of Jim Molsheim, John Field, Mario Silver, and Luis Sejo.
[Dr. Claudia Henschke] [177.19s] So this is these collaborations are very important, and we're we we appreciate all the hard work towards that.
[Dr. Claudia Henschke] [185.50s] We had worldwide registration over 400.
[Dr. Claudia Henschke] [188.06s] We hope to have even more at this meeting and in future meetings.
[Dr. Claudia Henschke] [192.76s] So the goals of our, 46 conference is to maximize the benefit of screening, and we need to keep rethinking and optimizing all components of both the diagnostic and the treatment paradigm to reach that 95% or maybe even higher.
[Dr. Claudia Henschke] [211.19s] We've done that by looking at all the organs that we see on the chest CT.
[Dr. Claudia Henschke] [216.94s] This time we're focusing we provide the information on the report of the nodule location, the size, and the change.
[Dr. Claudia Henschke] [236.00s] We provide the information on each of the visualized more organs in the chest, and we collaborate with relevant medical specialties and engineering experts to really get provide the correct information because in a screening setting is very different than in the usual clinical setting.
[Dr. Claudia Henschke] [255.23s] In screening, you're looking at a whole population.
[Dr. Claudia Henschke] [257.99s] You wanna be very careful what your recommendations are in order not to do harms.
[Dr. Claudia Henschke] [263.75s] And we've published in peer reviewed journals and I'll just review that a little bit prior to make on each topic prior to making recommendations.
[Dr. Claudia Henschke] [273.74s] So for coronary artery calcifications, we looked at that from early on, because we said we see those and we doctor Shemesh, who's here where are you, doctor Shemesh?
[Dr. Claudia Henschke] [285.50s] There you are.
[Dr. Claudia Henschke] [286.70s] Worked with us early on from, in in doing that.
[Dr. Claudia Henschke] [293.05s] We developed the ordinal scoring, CAC scoring.
[Dr. Claudia Henschke] [298.00s] So we said for an 4 arteries, we classify the calcifications as to none, mild, moderate, or severe.
[Dr. Claudia Henschke] [307.71s] That gives us a possible score from 0 to 12, and then we showed that, that having a score of 4 or more gave you an, an odds ratio of a hazard ratio of 2.1, compared to a score of lower.
[Dr. Claudia Henschke] [326.13s] So we make recommendations for each of those.
[Dr. Claudia Henschke] [329.73s] And radiology in 2010 when we published the, the second article on that said you they had an editorial where they quoted the 3 papers by that I listed here, Shemesh, Gondry, and Budoff that said these are things that we we can see on the CT.
[Dr. Claudia Henschke] [350.31s] We can quantify them, and the editorial said to radiologists, it's important to provide quantitative information, post processing information.
[Dr. Claudia Henschke] [360.14s] So I wanna really underscore that because we've been moving towards that and we need to do even more.
[Dr. Claudia Henschke] [367.79s] We looked at the agreement between the ordinal and the Agustin scores and we worked we also looked at never smokers because we did had a grant from the Flight Attendants Medical Research Institute.
[Dr. Claudia Henschke] [379.64s] Those are all those flight attendants who had that passive smoking exposure.
[Dr. Claudia Henschke] [384.29s] And in the second talk later today, I'll talk about the score that we developed for, the passive smoking exposure.
[Dr. Claudia Henschke] [391.81s] But we showed that if you have low, moderate, or high exposure, you have an increasing risk of coronary calcifications.
[Dr. Claudia Henschke] [400.94s] So that was a very important paper that was published.
[Dr. Claudia Henschke] [405.81s] We also looked at quantifying the extent of emphysema as you see here, and we said you can have mild, moderate, or severe, and we developed the hazard ratios for lung cancer, or for COPD survival.
[Dr. Claudia Henschke] [422.68s] If it's moderate emphysema, there was a hazard ratio of of 17.3, and for marked, it was 43.
[Dr. Claudia Henschke] [430.25s] So there's a mark marked prediction value of, emphysema and the quantification of emphysema.
[Dr. Claudia Henschke] [440.33s] We looked at emphysema phenotypes that if depending on the type of severity and and where it's located, that also provides additional information.
[Dr. Claudia Henschke] [451.75s] And we showed that when never smokers have emphysema, they're at the same risk of lung cancers as smokers, and that's something that's really not understood.
[Dr. Claudia Henschke] [461.69s] So quantifying the extent of the passive smoking exposure and knowing what the CT shows is very important.
[Dr. Claudia Henschke] [469.82s] We looked at aortic calcifications, and we score each of those as non mild, moderate, or severe in each of our reports.
[Dr. Claudia Henschke] [478.46s] The yellow that you see there is coronary calcium, aortic valve calcifications as compared to the pink, which is, mitral valve.
[Dr. Claudia Henschke] [488.08s] So you need to carefully distinguish them, and these are all things that are needed in the training of radiologists reading these scans or in the AI algorithms that are being developed.
[Dr. Claudia Henschke] [498.83s] We looked at the entire we talk about the entire aorta, whether it's how much calcification there is.
[Dr. Claudia Henschke] [507.47s] And then we look at the lungs.
[Dr. Claudia Henschke] [509.15s] We carefully evaluated bronchiectasis because we said if you can find that early, maybe we can intervene and keep it from, becoming worse.
[Dr. Claudia Henschke] [519.26s] And that's ongoing research that you'll hear about today as well.
[Dr. Claudia Henschke] [524.30s] We published lots of things about the liver because in the World Trade Center, which we have, we have the data and and we have experts, Andrea Branch, and you'll hear a talk by doctor Fried later.
[Dr. Claudia Henschke] [536.99s] These this is really an important finding and the correlation of the liver with heart, with lung, all of those things are unexplored.
[Dr. Claudia Henschke] [546.24s] So that's one of our one of our many goals.
[Dr. Claudia Henschke] [551.43s] We we reported on interstitial lung disease and breast parenchymal disease that you can see on low dose CT.
[Dr. Claudia Henschke] [558.32s] In fact, if you see the density readings, the agreement among mammographers is much better if you look at CT scans than the mammogram.
[Dr. Claudia Henschke] [569.30s] So we published on that.
[Dr. Claudia Henschke] [570.66s] And when you see, artery calcifications on a mammogram, we said that's predictive of coronary artery disease as well.
[Dr. Claudia Henschke] [579.55s] And then they said, oh, well, but women don't wanna know that from their from their mammogram.
[Dr. Claudia Henschke] [583.96s] They're focused on the breast.
[Dr. Claudia Henschke] [585.59s] And we had a survey.
[Dr. Claudia Henschke] [586.87s] Laurie Margulis, did a survey and said, of course, women wanna have that information.
[Dr. Claudia Henschke] [592.15s] So that's the answer to all that information that we we wanna get from the CT scan.
[Dr. Claudia Henschke] [599.04s] We looked at osteoporosis.
[Dr. Claudia Henschke] [602.96s] And back in 2017, together with Tony Reeves, who's sitting somewhere also in the in the audience, we said, well, we should have a digital report.
[Dr. Claudia Henschke] [613.54s] And we at that time, we had it for nodule detection, for growth, for emphysema, coronary artery calcifications, but we needed to further develop that.
[Dr. Claudia Henschke] [622.66s] And we've later on, we developed a more extensive quantitative, report.
[Dr. Claudia Henschke] [631.12s] And so the exciting thing about this meeting is that we're gonna extend expand that.
[Dr. Claudia Henschke] [636.07s] We're going to talk about chamber size, and Mort will talk about that.
[Dr. Claudia Henschke] [639.83s] He's done terrific work.
[Dr. Claudia Henschke] [642.57s] And really, we need to quantitate the osteoporosis in the liver and that's the focus of of this conference.
[Dr. Claudia Henschke] [650.09s] And really, that's bringing in an era of a new era of preventive health.
[Dr. Claudia Henschke] [656.69s] Really, we need to start thinking about it differently.
[Dr. Claudia Henschke] [659.82s] We need to think about health rather than illness.
[Dr. Claudia Henschke] [663.01s] So those are all exciting things for the future.
[Dr. Claudia Henschke] [666.77s] So the sun is rising on early diagnosis and early treatment, And we thank all of our ICAL CAP investigators and their teams throughout the world really from 1999 till today.
[Dr. Claudia Henschke] [679.03s] That's a long time and we and each and every one of those, investigators are important for us.
[Dr. Claudia Henschke] [685.67s] And special thanks to the thousands of screening participants that we have that have generously given us their data and allowed us to report on that.
[Dr. Claudia Henschke] [697.64s] So for the future, we have the next joint meeting with Agile, which is the European component from April 3rd to April 5th, next year in Bangkok.
[Dr. Claudia Henschke] [711.33s] We're at the, one of our fell previous fellows is is helping coordinate that.
[Dr. Claudia Henschke] [717.80s] She's a pulmonologist at at the Princess.
[Dr. Claudia Henschke] [723.73s] I can't really pronounce that name, but the College of Medicine in in Bangkok.
[Dr. Claudia Henschke] [731.06s] And then the next date, the the follow-up of this conference is going to be September 18th to 20th in New York City.
[Dr. Claudia Henschke] [739.86s] So we look forward to all sorts of new developments by then.
[Dr. Claudia Henschke] [744.46s] Thank you very much.
Transcript of Dr. Morteza Naghavi's Presentation:
Jump to Dr. Claudia Henschke's Introduction and Presentation
Jump to Dr. David Yankelevitz's Presentation
[Dr. Morteza Naghavi] [745.98s] Good morning, and welcome.
[Dr. Morteza Naghavi] [749.65s] This is truly a treasure type event crossing the, lung cancer screening world and cardiovascular prevention and early detection world.
[Dr. Morteza Naghavi] [762.97s] I come from, the cardiology side.
[Dr. Morteza Naghavi] [766.97s] I started SHAPE, Society For Attack Prevention and Eradication, which started from Wollamble plaque.org.
[Dr. Morteza Naghavi] [773.77s] And our notion was to go out and detect people before they become an acute coronary disease and symptomatic.
[Dr. Morteza Naghavi] [784.57s] When I met Claudia and David about 5 years ago, we thought that we were united with a chest CT scan.
[Dr. Morteza Naghavi] [794.18s] A chest CT scan has information both for cardiology side and for lung cancer screening.
[Dr. Morteza Naghavi] [799.22s] So we quickly evolved our thoughts.
[Dr. Morteza Naghavi] [802.26s] And what you will see, a quick overview of what we've accomplished in the past 2, 3 years.
[Dr. Morteza Naghavi] [807.23s] We went through, pandemic together.
[Dr. Morteza Naghavi] [810.35s] So, why are we here?
[Dr. Morteza Naghavi] [813.87s] The main element of our work is we are able noninvasively to detect early stage of CBD and lung cancer using a low dose CT scan.
[Dr. Morteza Naghavi] [825.72s] It is not a research tool anymore.
[Dr. Morteza Naghavi] [828.28s] It's a clinical tool widely available.
[Dr. Morteza Naghavi] [831.04s] It's available all the way in India and China and developing countries, and it's ready for mass adoption.
[Dr. Morteza Naghavi] [839.37s] And sorry.
[Dr. Morteza Naghavi] [842.40s] AI has made it possible to deliver it on a cost efficient human resource wise efficient and inexpensive manner.
[Dr. Morteza Naghavi] [852.94s] So those are the key momentum take makers that brought us here.
[Dr. Morteza Naghavi] [858.38s] But why do we have to do this?
[Dr. Morteza Naghavi] [861.83s] This is the grimest statistics that have been here, for over 200 years, at least during my decades in cardiology.
[Dr. Morteza Naghavi] [870.23s] And that is for coronary disease, for cardiovascular disease, we really don't have any early stage screening platform.
[Dr. Morteza Naghavi] [880.02s] We do screening for blood pressure.
[Dr. Morteza Naghavi] [882.18s] We do screening for hyperlipidemia and diabetes, but we don't have a screening for early detection of presymptomatic disease.
[Dr. Morteza Naghavi] [891.80s] And we just wait till somebody comes in with chest pain, and we throw everything we have at them.
[Dr. Morteza Naghavi] [898.04s] So these two statistics need to change in order for us to make a difference in primary prevention of the number 1 and number 2 killers.
[Dr. Morteza Naghavi] [908.60s] I wanna put something here.
[Dr. Morteza Naghavi] [910.36s] I'm sure, doctor Harrington has much more detailed slide to to share with you about the burden of cardiovascular disease.
[Dr. Morteza Naghavi] [919.26s] But we when we go to cardiology meetings over the last 20, 30 years, we're all used to seeing this graph.
[Dr. Morteza Naghavi] [925.58s] This is a misleading graph.
[Dr. Morteza Naghavi] [928.71s] This does not represent the burden of the disease.
[Dr. Morteza Naghavi] [932.47s] This is called age adjust.
[Dr. Morteza Naghavi] [934.47s] And I and I was in a school of public for a MPS program, so I I relate to that.
[Dr. Morteza Naghavi] [940.71s] But this is not reality.
[Dr. Morteza Naghavi] [942.87s] Because when you say age adjusted, that means you treat people or our society as if we stuck in the same age distribution of 1900.
[Dr. Morteza Naghavi] [952.63s] But we are getting older.
[Dr. Morteza Naghavi] [953.90s] The population is aging.
[Dr. Morteza Naghavi] [955.83s] And the real statistics is this aside.
[Dr. Morteza Naghavi] [959.16s] This is not age adjusted.
[Dr. Morteza Naghavi] [960.68s] This is the reality.
[Dr. Morteza Naghavi] [961.72s] And you can see the age adjusted are the red and and blue, but the reality of burden of disease keeps going up.
[Dr. Morteza Naghavi] [969.40s] And so that's the problem we're facing, and we need to make a difference.
[Dr. Morteza Naghavi] [974.27s] And that's worldwide.
[Dr. Morteza Naghavi] [976.20s] Wars in countries like China, Russia, and developing countries as well as in the US.
[Dr. Morteza Naghavi] [983.63s] So this is what we've been working on over the past 3, 4 years, particularly past 2 years, and we have some good success to share with you.
[Dr. Morteza Naghavi] [993.61s] Again, applying AI and new, innovative technologies to the CT scans.
[Dr. Morteza Naghavi] [1000.17s] The same work that Claudia and David started years ago, but combining it with cardiovascular is our focus.
[Dr. Morteza Naghavi] [1008.80s] And if we do it well, we can handle in and out time within 7 minutes.
[Dr. Morteza Naghavi] [1013.92s] And that's you'll see in the subsequent slides that we're proposing to ARPA to, fund this initiative, for nationwide implementation.
[Dr. Morteza Naghavi] [1024.30s] So the idea is we would make it widely available, particularly in mobile settings.
[Dr. Morteza Naghavi] [1029.98s] People go in and out there going for their grocery, shopping.
[Dr. Morteza Naghavi] [1033.74s] They can scan a QR code on the back of this truck.
[Dr. Morteza Naghavi] [1037.81s] They get the app.
[Dr. Morteza Naghavi] [1039.01s] They answer a few questions.
[Dr. Morteza Naghavi] [1041.01s] They, you know, totally, we have over 35,000,000 people that qualify according to our existing guidelines for for coronary artery calcium score in the intermediate group and for lung cancer screening.
[Dr. Morteza Naghavi] [1052.06s] And the AI does the initial reading and then radiology, or cardiology or any expert approves the report and then brings it to a nurse practitioner or a patient advocate or somebody who can walk the patient through, the findings.
[Dr. Morteza Naghavi] [1072.60s] So I don't wanna go into details of these as Claudia mentioned.
[Dr. Morteza Naghavi] [1076.34s] These are work that they have done.
[Dr. Morteza Naghavi] [1078.10s] We're just applying it to, an AI based reader and make it easily available through app and cloud.
[Dr. Morteza Naghavi] [1087.06s] So here's the thing.
[Dr. Morteza Naghavi] [1089.79s] The according to AHAACC guideline and the intermediate risk category group, we have about a little bit more than 35 now.
[Dr. Morteza Naghavi] [1098.99s] 35,000,000 people will qualify, would benefit from getting their calcium score.
[Dr. Morteza Naghavi] [1103.94s] The total number today is less than half a1000000.
[Dr. Morteza Naghavi] [1106.90s] We don't have even accurate statistics because it's not covered by Medicare.
[Dr. Morteza Naghavi] [1111.46s] So we don't have so this is the the the proposal.
[Dr. Morteza Naghavi] [1116.27s] On the right side, the lung scan will cover the entire lung, but for cardiovascular or calcium score, imaging, we only cover the the heart.
[Dr. Morteza Naghavi] [1126.51s] So we don't have guidelines to go above the cardiac for this 33 or 35,000,000.
[Dr. Morteza Naghavi] [1132.80s] That's one of the questions that we hope to discuss and bring to resolution or bring to an action plan for writing group, through this meeting.
[Dr. Morteza Naghavi] [1142.27s] So that was, the highlights.
[Dr. Morteza Naghavi] [1145.38s] About 25,000,000, you take out the lung population, especially with the expanded definition of lung cancer screening.
[Dr. Morteza Naghavi] [1153.14s] We need to answer that question whether that extra dose for the upper part, 1 third of the lung, is justifiable.
[Dr. Morteza Naghavi] [1160.77s] And I quote David, Ian Kalovich, who's the expert, he's telling me it's not gonna be more than one chest X-ray for this, amount of extra dose.
[Dr. Morteza Naghavi] [1172.29s] And, hopefully, we can convince our colleagues to stop doing things like this that where they just leave out part of the lung and not cover, you know, vertebral property and not cover the areas that the patient can get benefit from through the AI and getting, actionable information.
[Dr. Morteza Naghavi] [1190.66s] So first, we focus on what the US Preventive Task Force Services has actual mandate, osteoporosis screening.
[Dr. Morteza Naghavi] [1198.58s] The information is there.
[Dr. Morteza Naghavi] [1200.02s] No more radiation.
[Dr. Morteza Naghavi] [1201.14s] No more extra time.
[Dr. Morteza Naghavi] [1202.44s] So that's already FDA approved and is being propagated through systems to make it available.
[Dr. Morteza Naghavi] [1209.88s] Mount Sinai just got it, installed.
[Dr. Morteza Naghavi] [1213.72s] This is the newest evolution of what we're doing, and that is using the non contrast chest CT scan, cardiac scan, calcium score, and lung cancer screening.
[Dr. Morteza Naghavi] [1226.67s] We'd be able to use AI to measure the volume of cardiac chambers and alveolar mass.
[Dr. Morteza Naghavi] [1234.60s] And we have, over the past 2 years, shown that the data in the gated and nongated lung scan are very similar.
[Dr. Morteza Naghavi] [1244.39s] We published that the actual volume of LA left atrium can predict who will have atrial fibrillation, who will have atrial fibrillation, not having atrial fibrillation within a year.
[Dr. Morteza Naghavi] [1257.37s] And we showed that compared to a standard of care, like CHARGE AF, which is a risk calculator, the LA volume does a much better job in identifying who, is going to have atrial fibrillation.
[Dr. Morteza Naghavi] [1271.73s] And then thanks to MESA, a longitudinal study of 20 years where people went through calcium score and MRI, you can see the AI measures LV volume and LV mass very similarly to MRI.
[Dr. Morteza Naghavi] [1288.31s] And the AUC is total overlap.
[Dr. Morteza Naghavi] [1291.42s] No difference.
[Dr. Morteza Naghavi] [1293.35s] The same thing for predicting stroke, the AI and MRI.
[Dr. Morteza Naghavi] [1299.83s] Of course, MRI is, you know, 30 minutes or so time, whereas this is a matter of few seconds applying to existing scan, and you get opportunistically valuable information for predicting who will have a stroke and, atrial fibrillation.
[Dr. Morteza Naghavi] [1316.24s] So overall, we've shown that compared to the traditional Agasson score, this AI enabled and improved version increases the area under the curve significantly for all categories.
[Dr. Morteza Naghavi] [1330.42s] So that's what we're focusing on now and talking with FDA whether we can allow a bundle reporting like this.
[Dr. Morteza Naghavi] [1339.90s] Again, everything that Claudia and team over the past 25, 30 years pioneered in the lung cancer population, we bring it to the larger population that would qualify for cardiovascular screening and get a report like this that covers chambers, calcium, aorta, and so on.
[Dr. Morteza Naghavi] [1358.12s] So this is the final slide.
[Dr. Morteza Naghavi] [1360.68s] We're hoping that we can convince the new agency, ARPA h, just like DARPA.
[Dr. Morteza Naghavi] [1366.26s] This is ARPA for advanced research program agency for health.
[Dr. Morteza Naghavi] [1370.89s] They have mandates to make significant difference in health care.
[Dr. Morteza Naghavi] [1375.62s] They have, intention to create what they call moonshots.
[Dr. Morteza Naghavi] [1379.86s] So our proposal to them is to allow us in a foreseeable 5 to 10 years, have a 1,000 of these mobile units across the country in parking lots of retail, or organization like Walmart and Cargets and Kroger's.
[Dr. Morteza Naghavi] [1395.01s] It would be able to connect them through cloud and AI.
[Dr. Morteza Naghavi] [1398.68s] Half people, we go where people are, not waiting for them to come to hospitals and do the initial screening.
[Dr. Morteza Naghavi] [1406.18s] And with that, the approach is we'll be able to prevent preventable death.
[Dr. Morteza Naghavi] [1411.30s] Again, we may delay certain things, but we definitely can prevent the low hanging fruit with those people with very significant subclinical disease that have no idea and walk around.
[Dr. Morteza Naghavi] [1422.07s] So in summary, that is the proposal we're building on the back of this conference.
[Dr. Morteza Naghavi] [1427.27s] We hope to build the brainstorming that we come from, this meeting to what we call here reshaped, redefining screening for heart and pulmonary early disease.
[Dr. Morteza Naghavi] [1438.18s] These are my colleagues who have intellectually contributed to our work, and we look forward to publishing this after this meeting.
[Dr. Morteza Naghavi] [1445.57s] Thank you very much for coming early and participating in this event.
Transcript of Dr. David Yankelevitz's Presentation:
Jump to Dr. Claudia Henschke's Introduction and Presentation
Jump to Dr. Morteza Naghavi's Presentation
[Dr. David Yankelevitz] [1451.80s] I'm gonna present some of the details of this conference now, and then we'll get started.
[Dr. David Yankelevitz] [1458.30s] So I really believe that we are at the inflection point.
[Dr. David Yankelevitz] [1462.54s] Lung cancer screening has had a slow rise.
[Dr. David Yankelevitz] [1466.38s] But the idea that we're finally able to really start integrating now with cardiology in a in a really meaningful way, I think is gonna be like rocket fuel for this.
[Dr. David Yankelevitz] [1478.52s] And I I really think that this is gonna just enhance what's going on.
[Dr. David Yankelevitz] [1482.76s] I think there's a new era of preventive health that's about to happen.
[Dr. David Yankelevitz] [1487.09s] And I'm pleased to say that I think this conference our dream is that this conference will will really help make that happen.
[Dr. David Yankelevitz] [1496.21s] I wanna say also that Claudia just received recently, couple of weeks ago.
[Dr. David Yankelevitz] [1502.83s] She was given the, Joseph Cullen Prevention Award for early detection at the IASLC, the International Association For the Study of Lung Cancer.
[Dr. David Yankelevitz] [1512.83s] And, you know, there was a time, believe it or not, where lung cancer screening was controversial.
[Dr. David Yankelevitz] [1521.41s] It seems like, it never was a problem, but we're delighted that it's really moving into, mainstream.
[Dr. David Yankelevitz] [1527.89s] We have a lot of people here to thank for that, from the American College of Radiology, from American Cancer Society.
[Dr. David Yankelevitz] [1535.09s] All of these organizations, American Lung Association, who are here today.
[Dr. David Yankelevitz] [1539.40s] All of them have really helped in making lung cancer screening become a reality, and it's gradually improving.
[Dr. David Yankelevitz] [1545.59s] Uptake is increasing.
[Dr. David Yankelevitz] [1547.51s] And I I think this award that Claudia got is in large part recognition of that.
[Dr. David Yankelevitz] [1552.95s] Claudia mentioned this article.
[Dr. David Yankelevitz] [1554.31s] I just wanted to this was an editorial that came out in 2010, and it was based on these articles.
[Dr. David Yankelevitz] [1560.02s] And, actually, the first was the, osteoporosis, and that's integrated here.
[Dr. David Yankelevitz] [1566.34s] Matt Budoff's, approach is being integrated into what Mort is doing.
[Dr. David Yankelevitz] [1571.30s] Shemesh has worked with us with, Claudia, and we've integrated the ordinal scoring, and the third was, on thoracic, diseases and thoracic calcification.
[Dr. David Yankelevitz] [1582.91s] But the main point I wanted to bring out about this article was this is what they said, and this was really new at that time.
[Dr. David Yankelevitz] [1590.77s] In this issue of radiology, the idea of reporting all clinically relevant findings is taken to a new exciting and potentially more ambiguous level.
[Dr. David Yankelevitz] [1598.92s] In 3 separate studies, we discovered that radiologists may be able to offer even more clinically relevant information that is based not on what we see, not not on what we can see, but rather on what we cannot see, at least at first glance.
[Dr. David Yankelevitz] [1613.74s] These reports suggest a change in the paradigm for merely reporting the image findings to taking an extra analytical post processing step to create and report a numeric finding that may help to assess a patient's risk for cardiovascular disease or osteoporosis.
[Dr. David Yankelevitz] [1629.64s] The idea of doing this was new at that time, and, this is before the era of AI.
[Dr. David Yankelevitz] [1637.64s] I mean, it's really quite remarkable.
[Dr. David Yankelevitz] [1639.08s] And then they they noted that if these reported methods hold true, it's uncertain when and for whom such post processing analyses should be performed and reported.
[Dr. David Yankelevitz] [1649.42s] An even bigger problem today.
[Dr. David Yankelevitz] [1651.18s] This is gonna be one of the topics we discussed.
[Dr. David Yankelevitz] [1653.42s] There's lots of things that you can find on these CTs and and predict how we report it.
[Dr. David Yankelevitz] [1658.14s] Is it ethical to report?
[Dr. David Yankelevitz] [1659.64s] All of these are now becoming challenges.
[Dr. David Yankelevitz] [1662.20s] And finally, they concluded with this paradigm shift allows for a rich avenue for further research and development rather than shying away from this new responsibility.
[Dr. David Yankelevitz] [1671.52s] The radiology leadership should embrace the possibility of adding a new dimension to our profession.
[Dr. David Yankelevitz] [1677.68s] This is going to explode with AI.
[Dr. David Yankelevitz] [1679.85s] We have to figure out how to integrate this, but we feel that what we're doing now with with low dose CT of the chest, as Cheryl Hilton described at our last meeting, is a new era in preventive health, and I believe that.
[Dr. David Yankelevitz] [1694.96s] Our conference, day 1 is really an introduction of the cardiology world, and I'm happy to say we have the Stanford gang here is gonna help, educate us.
[Dr. David Yankelevitz] [1708.55s] But we have wonderful panel.
[Dr. David Yankelevitz] [1709.74s] They're gonna really bring out all of the issues in in cardiology that we feel, will be addressed in in these scans and how it's gonna be integrated.
[Dr. David Yankelevitz] [1719.46s] And then we bring in the lung the lung side of this, all of the illnesses in lung that are we're able to identify, and and discussions on on early early diagnosis leading to early treatment.
[Dr. David Yankelevitz] [1734.49s] So it's a bit of an introduction of the two worlds.
[Dr. David Yankelevitz] [1737.06s] And then finally, there's a third section here on other findings, especially that and they relate liver disease, fat distributions, all of this interplays with all of these illnesses.
[Dr. David Yankelevitz] [1748.35s] Day 2 is how we work together, basically.
[Dr. David Yankelevitz] [1751.35s] How we build a common protocol, make it really efficient, how we optimize performing these together, and then there'll be issues related to some of the ethical considerations and also how organizations, advocacy organizations work together.
[Dr. David Yankelevitz] [1770.24s] You know, they've been siloed.
[Dr. David Yankelevitz] [1772.24s] There's lung there's cancer advocacy, there's cardiac advocacy.
[Dr. David Yankelevitz] [1775.68s] How do they work together?
[Dr. David Yankelevitz] [1776.88s] We've got to think of this in a much broader way.
[Dr. David Yankelevitz] [1781.82s] And on day 3 whoops.
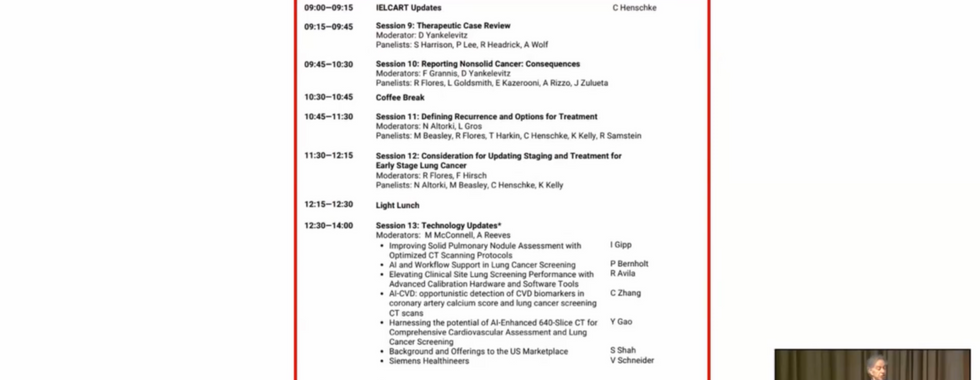
[Dr. David Yankelevitz] [1785.41s] Day 3 is primarily, on lung cancer treatment, and that's our Elkhart program, and we'll be talking about opportunities for treatment and improving treatment of lung cancer.
[Dr. David Yankelevitz] [1798.51s] And we'll also give some technology updates, and doctor Fuster is gonna close off the meeting with a 45 minute lecture on cardiology, which we're delighted about.
[Dr. David Yankelevitz] [1810.02s] So that's the program.
[Dr. David Yankelevitz] [1813.14s] We have lunch here every day where everybody is free for dinner tonight.
[Dr. David Yankelevitz] [1816.83s] When people come to New York City, they have their favorite restaurants.
[Dr. David Yankelevitz] [1820.98s] People in this room will meet each other, and and choose where they wanna go.
[Dr. David Yankelevitz] [1827.05s] Friday night, we do have a special event, which I will get to in a moment.
[Dr. David Yankelevitz] [1832.57s] I wanna first acknowledge the conference sponsors, the City of New York Research Foundation, GE Healthcare, Bristol Myers Squibb, and Bristol Myers Squibb Foundation, Siemens, AstraZeneca, Araneta, United Imaging, Lilly, CELIO, Acumentra, and Claudia's Research Foundation.
[Dr. David Yankelevitz] [1852.67s] And finally, we have supporters, the International Association For the Study of Lung Cancer, Prevent Cancer Foundation, American Lung Association, and the Go to Foundation, as well as SHAPE and I LCAP are all supporters of this meeting.
[Dr. David Yankelevitz] [1866.63s] So we really appreciate all of this sponsorship and support.
[Dr. David Yankelevitz] [1872.72s] 2 other additional announcements.
[Dr. David Yankelevitz] [1874.88s] We are delighted that, we have Bruce Ratna here who recently published this book, Early Detection, Catching Cancers When It's Curable.
[Dr. David Yankelevitz] [1882.95s] This is a wonderful book.
[Dr. David Yankelevitz] [1885.03s] This goes into the I into the ideas of screening.
[Dr. David Yankelevitz] [1888.15s] Bruce was motivated through family history, to write this book.
[Dr. David Yankelevitz] [1893.29s] It's a wonderful read, and we are delighted that we have copies of the book here available to the audience members.
[Dr. David Yankelevitz] [1900.88s] And I urge you to take it and read this book carefully.
[Dr. David Yankelevitz] [1903.85s] It really brings out the history of screening, why it's so important, and where this needs to go.
[Dr. David Yankelevitz] [1909.57s] And we also have this book, which is written by Mike McConnell, fight heart disease like cancer.
[Dr. David Yankelevitz] [1916.77s] This is one of the best covers I've ever seen, I have to tell you.
[Dr. David Yankelevitz] [1921.03s] And Mike too was motivated by family history of illness and and how it should be how we should think about fighting heart disease, and he's using the the cancer paradigm to help with that.
[Dr. David Yankelevitz] [1931.84s] And I think this is also a wonderful book, and we have copies of this book here as well.
[Dr. David Yankelevitz] [1935.96s] So I really urge people to take these books and read them, and the authors are both here.
[Dr. David Yankelevitz] [1940.60s] I hope you get a chance to speak with them.
[Dr. David Yankelevitz] [1943.96s] As I said, this is this is I think it's just wonderful.
[Dr. David Yankelevitz] [1947.48s] This is the direction we need to head in preventive health.
[Dr. David Yankelevitz] [1951.89s] I mentioned that, there will be a reception tomorrow night at Claudia's house.
[Dr. David Yankelevitz] [1956.69s] This really isn't Claudia's house, by the way.
[Dr. David Yankelevitz] [1960.05s] In case you were confused, you might think it is, but this is a couple of blocks away from Claudia's house.
[Dr. David Yankelevitz] [1967.74s] But, we have live entertainment.
[Dr. David Yankelevitz] [1971.10s] Isabelle Stein, if some of you may remember, she presented.
[Dr. David Yankelevitz] [1974.14s] She performed at at one of our meetings about a year ago.
[Dr. David Yankelevitz] [1977.66s] She's a wonderful jazz singer, and and it'll be a lot of fun.
[Dr. David Yankelevitz] [1980.94s] This is on Friday night, and it's light food being served, and you can go out to dinner afterwards.
[Dr. David Yankelevitz] [1987.47s] And finally, I'm just gonna end with this slide.
[Dr. David Yankelevitz] [1990.43s] These are the terms we use for all of these find when we read a CT scan, we talk about coronary calcium as an ancillary finding or emphysema or all this ancillary, opportunistic, incidental, newer term, bonus, opportunity, and just look at their definitions, ancillary, subordinate, or subsidiary.
[Dr. David Yankelevitz] [2010.27s] You know, I don't think of the coronary calcium findings as subordinate or subsidiary, opportunistic, exploiting opportunities with little regard for principle, incidental, being likely to ensue as a chance or minor consequence, etcetera.
[Dr. David Yankelevitz] [2025.36s] So I think we have to get rid of this terminology.
[Dr. David Yankelevitz] [2028.56s] I I really don't like it, and I was talking to my colleague, doctor Mulshein, a former provost at Rush University, and he said that we really have to start thinking more what was the word we used, Jim?
[Dr. David Yankelevitz] [2044.66s] Yeah.
[Dr. David Yankelevitz] [2044.99s] That we have to talk not about lung cancer screening.
[Dr. David Yankelevitz] [2047.79s] It's really an opportunity for preventive health.
[Dr. David Yankelevitz] [2050.66s] And all of this all of these findings, none is subordinate to the other.
[Dr. David Yankelevitz] [2054.49s] None is incidental to the other.
[Dr. David Yankelevitz] [2056.41s] And so we've just gotta make it that this is a much more holistic approach, and I think we'll come up with some new terminology for how we describe the scan, not calling it a lung screening scan.
[Dr. David Yankelevitz] [2066.97s] It's an opportunity for preventive health on on these major comorbidities or morbidities that are all seen at the same time.
[Dr. David Yankelevitz] [2074.72s] And I think we've got to move in that direction.
[Dr. David Yankelevitz] [2077.36s] And with that, we're gonna have our first speaker and and doctor Marin, you're gonna introduce him.
[Dr. David Yankelevitz] [2085.44s] Thank you.
The presentations were hosted by I-ELCAP – The International Early Lung Cancer Action Program.


Comments